|
|
|
Submitted by Martin Jacobson, D.C., P. A. Marty plays in
the Palm Bay Senior League and is a Chiropractic Physician
SPORTS INJURY CORNER:
As
we all know, playing senior softball is a lot of fun, but, as most of us have
already experienced, there can be a lot of heartbreak also. The attrition rate
due to injury is very high and I'm sure the amount of Advil and Naprosyn
consumed by senior softball players is helping to keep Walgreen’s in business.
Unfortunately,
many of the aches and pains we all experience are unavoidable because we're
playing a very demanding sport with bodies that, to some degree, have lost
flexibility and strength because of deconditioning and the aging process. However, for those of us interested in
playing to the best of our present abilities, as well as prolonging our playing
days, there are options.
First
of all, it should be understood that if you simply show up on game days without
any physical preparation during the week, you probably will not approach your
potential as a player and your chances for debilitating injury will be great.
Seniors who are just returning to the game after not playing for many years are
especially at great risk for injury.
Too
many times we have seen new players injure themselves early in their first
season and never recover. Muscles that have not been subjected to the stresses
of softball are suddenly being asked to propel the player around the bases and
that player, not wanting to disappoint himself or his teammates pushes himself
beyond safe limits. He then limps or is
carried into the dugout and this very often is the end of his senior softball
career. This is sad for the player but
also sad for his teammates and the rest of the league. Our goal in managing our league is to
incorporate and encourage as many new players as we can. As most of us know, there's something
addictive and intoxicating about playing senior softball and it is always
enjoyable to see new players become part of our group.
What
I would like to do in these articles, is to share some of my knowledge and
expertise in regard to conditioning and rehabilitation so that we can perhaps
prevent some of these disabling and career ending injuries that we see happen
all too frequently.
As
a young person, I never was too concerned with warming up prior to playing and
can't recall suffering pulled muscles or aching bones. Now as a 60 year old, I can hardly move
unless I warm up for 20 minutes before playing.
Everyone should have their own routine to prepare themselves for
playing. If you're having problems with
your legs you might need to spend additional time getting them warmed up and
stretched so you will be ready to run when the game starts. Cold muscles will be much more prone to
injury than muscles that have been activated and warmed up through some
repetitive exercise.
I
think a key to pre-game warm-ups should be going through some of the movements
that you will have to do during the game.
I have noticed that one thing most of us have trouble doing is reaching
down to catch a ball while moving. This
requires not only coordination and flexibility but muscles strong enough to
support us while we lean forward. Doing forward and side lunges helps to
develop and strengthen our thigh and abdominal muscles which are very important
in those movements.
There
are numerous web sites that we can use to see illustrations and explanations
for different exercise. One web site
that I find helpful is www.coreperformance.com.
They have developed training regimens for athletes, as well as the average
person, that are helpful in improving our movement capabilities. As you can
tell from the name of that web site, they focus on development of the core
muscle groups which are very important in athletic movement.
SHOULDER INJURIES
One
of the most common maladies we deal with as senior softball players is pain and
stiffness in our shoulders, especially in the shoulder we use to throw. Many players must undergo surgery because of
injuries to their rotator cuff. But even
those of us who don't require surgery will often have trouble throwing or
experience some level of pain while throwing.
There
are many reasons for this and most of them relate to the degenerative affects of aging.
Often there are arthritic changes in the acromioclavicular (AC) joint
that can not only cause discomfort in the joint but contribute to impingement
and abrasion of the rotator cuff tendons. The rotator cuff is actually a point
of attachment in our shoulder of those tendons that are involved in lifting the
arm as well as holding the shoulder joint together. Tendonosis, or
tendon degeneration, occurs often in the rotator cuff tendons because of the
decreased circulation in that region.
Over the course of our lifetime our tendons in that area become weaker
because of the almost constant stress we put on our shoulders. Even as we stand or walk, the weight of our
arms is putting stress on those tendons in the shoulder region. If we work with our arms over our head, this
often results in compression of the tendons within the shoulder region. Also, we may have suffered some trauma that
has resulted in structural damage to the shoulder joints. Most of our tendon related problems, however,
are the result of chronic degeneration related to frequent micro trauma,
leading to a gradual weakening of the tissue that makes up the tendons. Remember, tendons are the attachment points
of muscle to bone.
As
senior softball players, we obviously are very vulnerable to these types of
shoulder problems because of our age, and the wear and tear we have experienced
over our lifetimes. Prevention of injury
should be our first concern. Therefore,
adequate warm-up and good mechanics are very important in prevention of
shoulder injuries. By warming up
adequately, we bring more blood into those tissues and allow for greater
flexibility. Cold muscles and tendons
will be more inflexible and more vulnerable for injury. In addition to simply playing catch prior to
game activity, the use of elastic tubing along with exercises performed with
dumbbells can be very helpful in strengthening our shoulder muscles and tendons
to help prepare us for the stresses of actual games.
A
comprehensive orthopedic shoulder evaluation will test for active and passive ranges
of motion as well as grade all muscles in the shoulder region for
strength. A determination can be made
whether the problem is related to muscle and tendon (contractile tissue) or (noncontractile tissue) bone, ligament or cartilage. MRI
studies of the shoulder can detect tendon tears as well as other types of
structural damage. X-ray studies
primarily are used to evaluate the bony structures of the shoulder for evidence
of arthritic changes, fracture, dislocation or pathology.
Treatment
options for shoulder injuries include surgery, steroid injections, rest, as
well as soft tissue treatments intended to promote healing of the injured or
degenerative tissue. If tendons are
completely torn surgery might be the best option, but for less severe conditions
conservative treatment should always be considered. Corticosteroid injections
are used to decrease inflammation in tissues, but do not stimulate healing of
tissue. Studies have shown an increased
incidence of tendon rupture subsequent to corticosteroid injections.
ACHILLES TENDONOSIS
Previously
referred to as Achilles tendinitis, this is a problem involving injury to the
tendons in the lower leg and will often involve pain in the heel and back of
the foot, which is where the tendons that allow us to stand on our toes,
attach. It is a common problem with
runners and others who participate in athletic activities. Individuals who
spend a great amount of time on their feet while working can also develop this
problem. It can become a chronic problem
that will often improve with rest and then return when strenuous activity is
resumed.
The
term tendonosis describes a chronic degenerative
condition involving a tendon. The term
tendinitis implies an inflammatory process involving a tendon, which is sometimes
seen following an acute injury. When a
condition becomes painful due to long-term stress on tissue, it is described as
tendonosis.
Conditions
such as overpronation (fallen arches or flat feet)
can also predispose a person to this problem.
Frequently, orthotics which are placed in the patient’s shoes can
provide support which reduces some of the stress on the foot and leg. Additionally, a method of treatment that
involves eccentric contraction of the tendon has been developed that has proven
to be very effective.
The
treatment involves the patient standing on the edge of a step and rising up on
his toes and slowly dropping down allowing his weight stretch the Achilles'
tendon against resistance. This can be
repeated in sets of 15 repetitions, up to 3 times, twice daily. They can be
initially performed with a straight knee, and then performed again with a
slightly flexed knee. These exercises
will be performed eight to 12 weeks. The patient should gradually add weight to
increase the stress on the tendon. This
can be accomplished by utilizing a backpack to which weights are added
incrementally.
Wearing
a heel lift in both shoes can also be helpful, and that it takes pressure off
of the tendon by flexing the foot slightly.
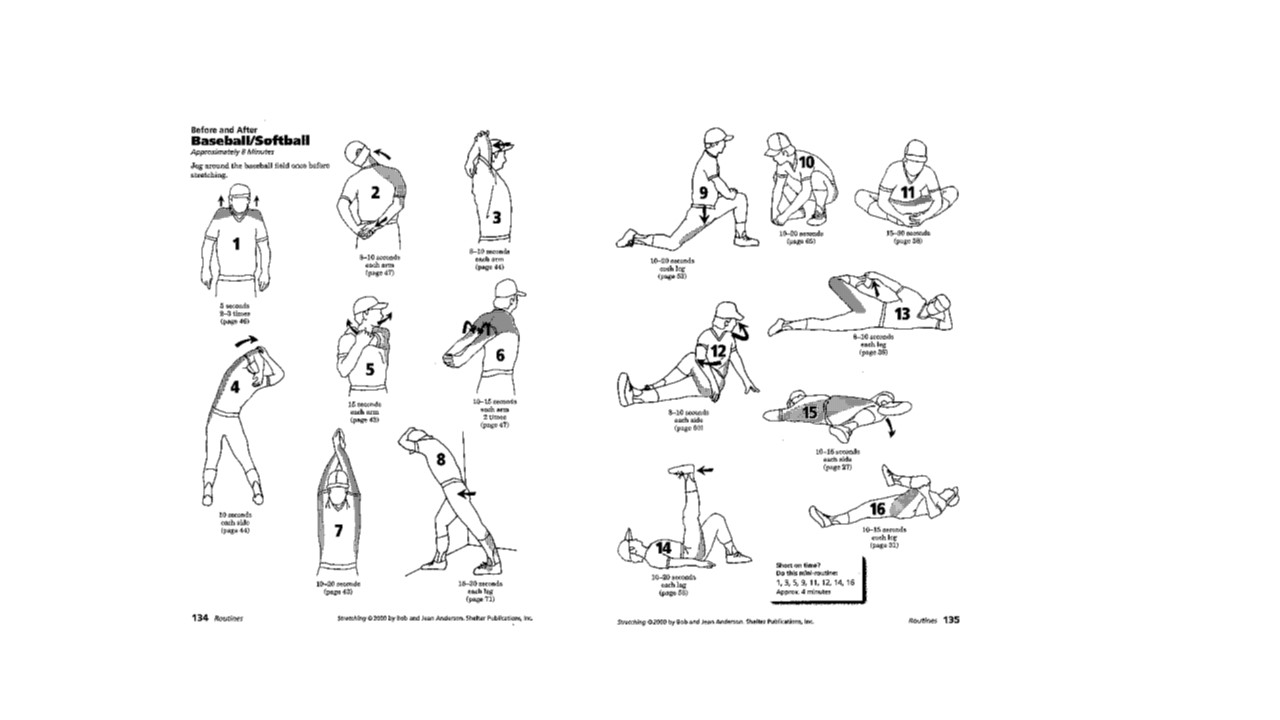
Game
day warm-up stretching exercises include sitting on the floor with your legs
straight out from you. Using a towel
wrapped around your toes or upper foot, stretch the foot back and hold for
20-30 seconds. Repeat this 2-3 times
per foot. This helps loosen the
tendons and muscles of the leg, foot and heel.
Many people have also found that their shoes are the problem – arch
locations differ in different shoes and orthitic
inserts can help make sure the arch has plenty of support.
Stretching Exercises